Whether you live in a state with strict stay at home orders from your governor or are still going about your life with few adjustments other than social distancing and more frequent hand washing, your life has  changed.
changed.
You may be an essential worker reporting to your workplace each day or adapting the best you can to working from home or fearing a layoff or already out of a job at this point.
You may have elder parents living with you or other family members with health issues that make them high risk.
Regardless, your life has changed. The fears, uncertainty, anger, sadness, exhaustion, confusion, and so many other emotions and feelings are real. We all have them.
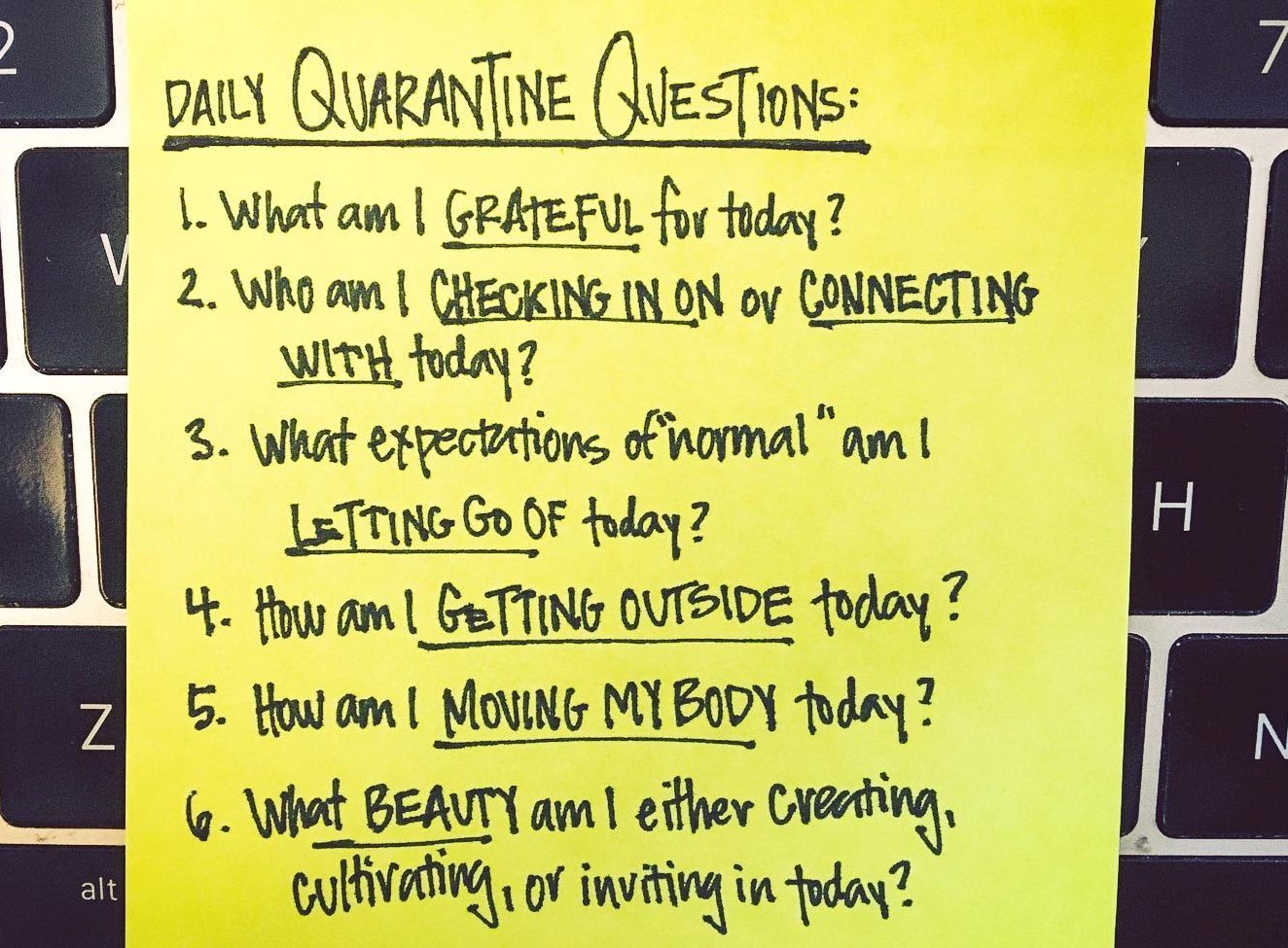
Self-care is important for all of us. As a CIO/CMIO colleague keeps telling his team, it’s a marathon not a sprint. The image I used this week is one of my favorites shared on Facebook by Brooke Anderson, a photographer in California. It’s a good reminder of how we need to take care of ourselves..
Here’s what my daily life looks like now:
- Staying at home: My husband and I haven’t been anywhere in 2 weeks except for when I picked up takeout at a local restaurant over a week ago.
- Working from home: Splitting time between our StarBridge Advisors business and work with a health system client on a variety of projects.
- Exercise: Walking our two little dogs and trying to get 10K steps each day keeping appropriate social distance with all the other walkers. There is a joy in seeing the spring flowers and buds on trees change each day – gives me hope!
- Family connection: Talking to my sister in Minnesota where I grew up and where all my three siblings and their families live. Keeping in touch with my daughters and their changed lives. One daughter is a Nurse Practitioner who will soon be caring for COVID-19 patients while her husband adapts to working full-time from home and their 3 and 5-year-old kids play together. The other daughter was already working from home; her husband is adapting to working from home while their first grader is doing the eLearning school program and their 5-year-old plays.
- Sharing resources: It’s hard to not be in the thick of it knowing what healthcare organizations are going through and how IT teams are working hard to support them. I’m channeling that energy into supporting Bill Russell and “This Week in Health IT” with a growing number of free COVID-19 resources for health IT teams.
- Social media with a purpose: I try to share what is most informative and useful as well as positive and motivating.
- Managing how much news I watch: On my busiest workdays I only watch at night. On more flexible days, I get snippets mid-day. In the spirit of being positive, I will say that the leadership demonstrated by New York Governor Andrew Cuomo is the leadership we need at all levels of government – fact based, informed, action oriented, and empathic.
And as the days blend together, the weekly routine now includes a couple new things. We gratefully receive grocery delivery that our nearby daughter has helped coordinate. We do a weekly family video call where the four grandkids stick their face right up to the camera and call out to their cousins then eventually go play so the six adults can talk and check in with each other. And we make a quiet moment to do Sunday online church which are YouTube messages from our ministers that we can watch anytime.
No matter what your days look like now, practice self-care. There are many resources out there to support you. The latest This Week in Health IT podcast – “Mental Wellness During Crisis” with Dana Udall PhD, Chief Clinical Officer at Ginger is definitely worth listening to.
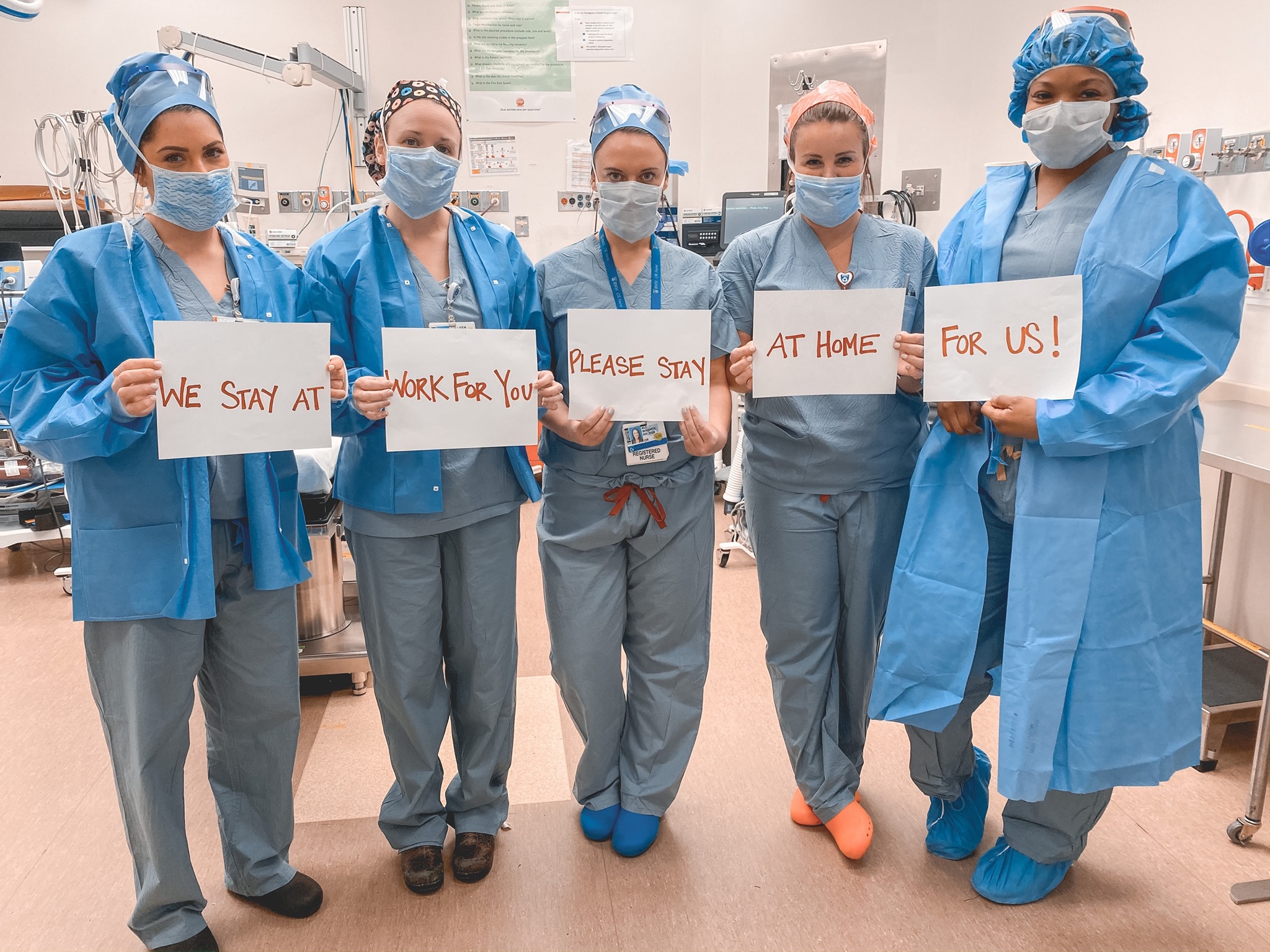
Whatever you might fear or feel inconvenienced by during this pandemic, think about the healthcare workers who like firemen run into the burning building, not away from it. They are going to work so we can stay home. They and all the essential workers who are keeping things running are the true heroes. To them I say thank you, be safe and well. To all of you, take care of yourself and those you love. We will get through this – together.

 close and without masks at a pool in Missouri, on the boardwalk in New Jersey and at a race track in North Carolina were concerning. As I hope many others chose to do, we stayed home and had a family visit on our patio at a social distance.
close and without masks at a pool in Missouri, on the boardwalk in New Jersey and at a race track in North Carolina were concerning. As I hope many others chose to do, we stayed home and had a family visit on our patio at a social distance.